


Tammy Bradly
Senior Director, Clinical Strategy and Market Insights
How Older Workers Are Reshaping Workforce Risk, Workers’ Compensation and Return-to-Work Strategy
The U.S. workforce is aging. This isn’t a temporary blip, it’s a long-term demographic shift that employers need to plan for. BLS (Bureau of Labor Statistics) projects labor force participation will continue rising among older workers through 2034, from 65.9% to 68.6% for workers ages 55–64, from 27.1% to 29.6% for ages 65–74, and from 8.6% to 10.2% for workers 75 and older.
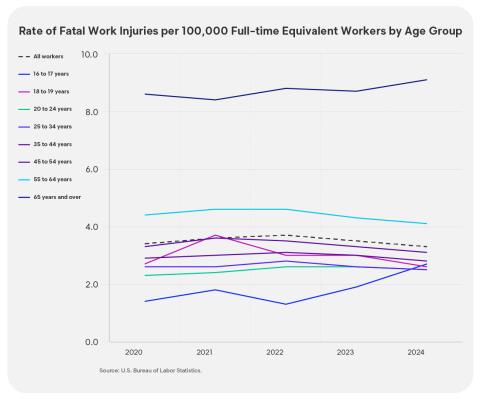
Older workers change the nature of workforce risk. The Centers Disease Control (CDC) notes that older workers generally have fewer nonfatal injuries than younger workers, but their injuries are more likely to be serious and fatal, and older workers often need more time to heal.
For workers’ comp, the bigger issue is claim severity and duration, not claim volume, that drives higher costs per claim
Employers and claims organizations will need stronger ergonomic design, earlier clinical coordination, better management of comorbidities, and more deliberate return-to-work planning to keep experienced employees working safely and control claim cost when injuries occur.

The Retirement Timeline Has Shifted: More People Are Working Longer
For years employers could assume that most workers would leave the labor force around traditional retirement age. That assumption no longer holds. More Americans are working later into life because of economic pressures, longer life expectancy, and a desire to stay engaged and productive.
This shift matters well beyond office settings. BLS’ latest employer-reported injury release shows that overexertion, repetitive motion, bodily conditions, and falls remain among the leading sources of serious workplace cases. These exposures are especially relevant in sectors where aging workers continue to play a large role, including manufacturing, health care, retail, transportation and construction.
The central question is not whether older workers belong in the workforce. They do, and they often bring experience, judgment and institutional knowledge. The real question is whether prevention programs, job design, and workers’ compensation strategies have kept up with the realities of an aging workforce. CDC’s guidance is explicit that employers should support and protect the health and safety of workers, especially those of advanced age.
Older Workers will Make Up More of the Workforce in the Next Decade
BLS projects participation rates will rise in each older age band through 2034, with especially notable increases among workers 65–74 and 75 and older. That means employers should expect a larger share of their workforce to be in age groups where recovery can be slower and the consequences of injury more serious.
CDC reinforces that, as the workforce continues to age, more claims will involve older employees even if injury rates decline overall. It also notes that the continued rise of older workers will require more tailored prevention strategies, especially ergonomic interventions and stronger return-to-work planning.
This is why workforce age mix is no longer just a demographic footnote. It is an operating condition that can affect disability duration, medical utilization and total cost of risk.

Why the Aging Workforce Matters to Employers and Risk Leaders
An injured employee’s recovery profile changes with age. Wear and tear on aging joints can increase susceptibility to musculoskeletal injury, while falls may become more consequential because of declining balance, depth perception, strength, vision and hearing.
This combination creates a different kind of risk. When injuries happen, they are more likely to intersect with degeneration, chronic disease, or functional limitations that make the claim harder to resolve.
Injury Patterns That Matter Most
Injury severity is the most important workers’ comp question for older workers. Several injury categories deserve special attention in an aging workforce. Falls, slips, and trips remain a major concern. BLS reported 721,720 DART (Days Away, Restricted, or Transferred) cases tied to falls, slips, and trips over the 2023–2024 period, with relatively long median case durations.
Overexertion, repetitive motion, and bodily conditions are even larger drivers of serious workplace cases. BLS reported 946,290 DART cases in that category over the same two-year period, the highest of any event or exposure group.
Older workers are more likely to experience musculoskeletal injuries and falls, and injuries such as rotator cuff tears, knee damage, back injuries, and degenerative aggravations become more common with age.
What Complicates Recovery and Return to Work
Chronological age alone does not explain why older-worker claims are harder to resolve. The complication usually comes from slower healing, chronic conditions, deconditioning, and a mismatch between medical improvement and actual job demands.
Comorbidities play a big role here. Chronic illnesses can complicate recovery and a WCRI study reported that 21% of workers’ comp claims had at least one comorbid condition, with costs more than double comparable claims. The same source argues that these health factors can slow recovery and complicate return to work across demographics, but especially among older workers.
Older workers often require more comprehensive care, more extensive treatment, and longer recovery, and may need gradual return-to-work plans or lighter-duty assignments instead of immediate full-duty release.
A Case Study in Severity: Joint Replacement
Joint replacement is one of the clearest examples of how aging workforce dynamics can affect workers’ compensation severity.
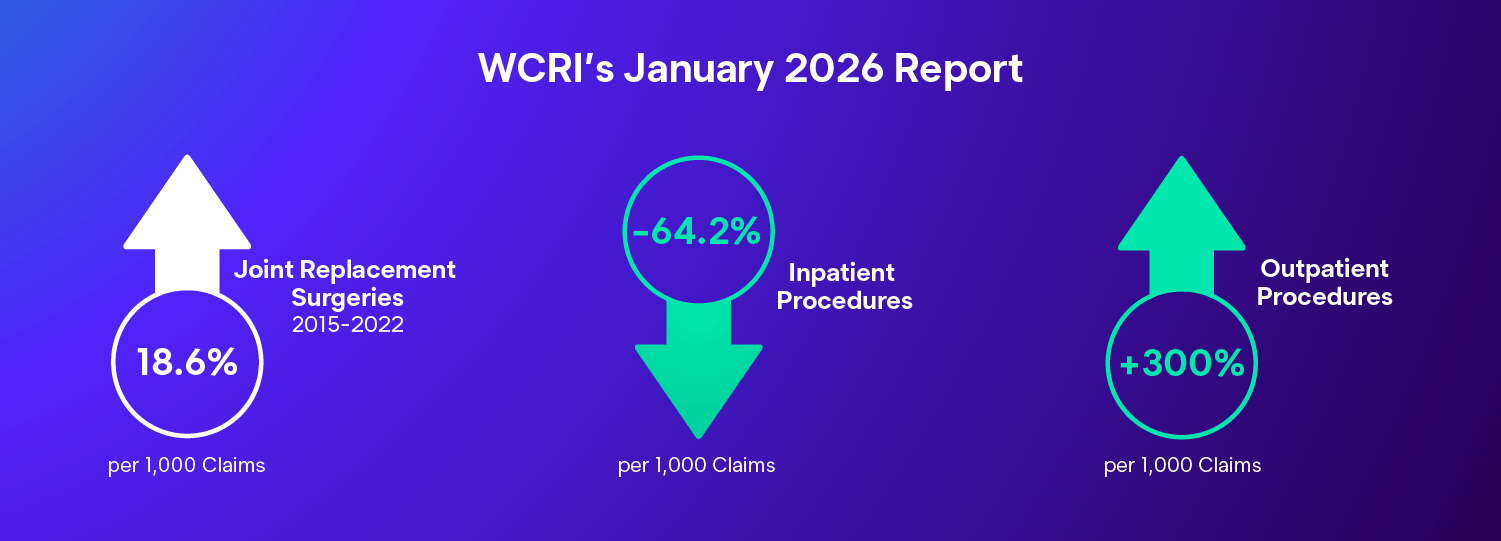
WCRI’s January 2026 report found that the number of claims with joint replacement surgeries increased from 7.0 to 8.3 per 1,000 claims between 2015 and 2022, while inpatient procedures fell from 5.3 to 1.9 per 1,000 claims and outpatient procedures rose from 1.6 to 6.4 per 1,000 claims. WCRI also found these claims carried total costs of $116,000 to $129,000 per claim, with temporary disability durations ranging from 43 to 55 weeks.
WCRI further found that joint replacement surgeries were highly concentrated among older workers. Three-quarters of workers with joint replacement surgeries were age 55 or older, and shoulder replacement cases skewed older still, with 86% age 55 or older.
The report also states that older workers and those with osteoarthritis were more likely to undergo joint replacement surgeries, and suggests health promotion, early intervention, and musculoskeletal wellness programs aimed at preserving function and preventing disability.
This makes joint replacement a useful case study because it sits at the intersection of age, degeneration, treatment intensity, disability duration and return-to-work complexity.

What Employers Can Do to Prevent Injury
The best prevention strategies are age-inclusive rather than age-exclusive. CDC recommends adapting work conditions to support older workers and emphasizes the value of designing work so people can remain healthy and productive across the life span. It recommends understanding workforce age distribution and job demands, then using that information to build programs that address both prevention and more complex injury management. It also highlights ergonomic and physical considerations, health risk assessments, screenings, behavior-change programs and broader wellness initiatives that benefit workers of all ages.
The goal is not to single out older workers as a liability. The goal is to reduce the mismatch between the worker and the work through better design, better equipment and better overall health support. Doing this supports all workers, regardless of age.

How to Change Claim Management to Be Age-Inclusive
Claims involving older workers usually aren’t about how often injuries happen, but about how serious, complicated, and long-lasting they are. Claim teams need earlier decision points and tighter coordination to prevent predictable delays from turning into avoidable disability duration.
Start with targeted triage. Use escalation criteria that combine age with known claim patterns to trigger earlier clinical involvement for higher-risk cases (for example, shoulder injuries over age 55). The goal is not to over-manage every claim; it is to surface likely duration drivers early before the claim becomes chronic and expensive.
Once a claim is escalated, clinical direction should be explicit: apply comorbidity-aware care pathways, reconcile medications, set functional milestones, and coordinate quickly across providers. These steps address the common severity drivers in older-worker claims such as slower healing, comorbidities, functional decline, unclear modified duty, and delays in coordination.
Treat return to work as the primary cost lever. When modified duty is unclear or delayed, indemnity duration expands quickly. That makes return to work a front-end strategy: secure work capabilities early, translate them into specific job tasks, and partner with the employer to place the worker into realistic transitional duty before the claim drifts.
Manage utilization earlier and more deliberately. These claims often include more diagnostics and longer physical therapy, and they carry a higher risk of over utilization when care is not guided by clinically sound medical utilization guidelines. Assign case management sooner, coordinate among specialists, and keep treatment anchored to measurable functional progress rather than extending passive care that does not move the employee toward work.
Identify barriers that sit outside the injury itself. Comorbidities, deconditioning, multiple medications, and psychosocial issues often explain why recovery lags. Case managers can shorten duration by surfacing these factors early, reconciling medications, confirming that underlying conditions are being managed, and helping the injured employee connect overall health to recovery even when the compensable injury is straightforward.
Clinical programs should reinforce a whole-person model by integrating physical and psychosocial supports, recognizing degenerative or age-associated conditions, and maintaining clear expectations for functional recovery. The objective is consistency: fewer handoffs, fewer delays, and clearer direction from injury through work re-entry.
Return to Work as a Front-End Strategy for Employers
Return-to-work planning should begin before the injury happens. Treat return-to-work planning as part of the recovery process, using job analysis, transitional duty and ergonomic assessment to identify ways to return the injured worker safely. Transitional duty can help employers retain access to the skills and expertise of experienced workers while easing them back into the workforce in a safe and timely manner.
That makes return to work a front-end strategy rather than a closing step. In an aging workforce, organizations that pre-plan transitional duty, workstation changes and realistic supervisor expectations will almost always outperform those that wait until the end of a claim to think about work re-entry.
The aging workforce is already reshaping workforce risk and workers’ compensation. While older workers are not necessarily injured more often, when injuries occur, the claims are often more severe, more medically complex, and harder to resolve. The right response is adaptation. Employers should redesign work, invest in ergonomic and fall prevention, and build return-to-work pathways before injuries happen. Claims organizations should treat older-worker claims as a signal for earlier clinical coordination, more realistic functional planning, and stronger recovery management.